Translation of "insufficient control" into Chinese. Monitoring the work of employees: types, methods, mistakes Insufficient control over activities
Russian
English
Arabic German English Spanish French Hebrew Italian Japanese Dutch Polish Portuguese Romanian Russian Turkish
Based on your request, these examples may contain crude language.
Based on your request, these examples may contain colloquial language.
Translation of "insufficient control" in Chinese
lack of control
Noun
(6 examples containing translation)
"lang="en">
Lack of control
View examples with translation insufficient monitoring
(7 examples containing translation)
" lang="en"> insufficient monitoring
View examples with translation inadequate control
" lang="en"> inadequate control
View examples with translation inadequate monitoring
(4 examples containing translation)
" lang="en"> inadequate monitoring
View examples with translation lack of monitoring
(4 examples containing translation)
" lang="en"> lack of monitoring
View examples with translation insufficient control
(4 examples containing translation)
" lang="en"> insufficient control
View examples with translation inadequate supervision
(3 examples containing translation)
" lang="en"> inadequate supervision
View examples with translation inadequate follow-up
(2 examples containing translation)
" lang="en"> inadequate follow-up
Other translations
Lack of resources and insufficient control water use give rise to conflicts between consumers.
Lack of control of water use is resulting in conflicts between users.">
The causes of poverty include high population growth, slow economic growth, social exclusion, insecurity and insufficient control for production assets.
The causes of poverty include high population growth rate, slow growth of economy, social exclusion, insecurity, and lack of control over productive assets.
Lack of control over productive assets.">
There is also concern insufficient control for the placement of children in childcare institutions and the insufficient number of qualified personnel working in this area.
Concern is also expressed about the insufficient monitoring of placements and the limited number of qualified personnel in this field.
Insufficient monitoring of placements and the limited number of qualified personnel in this field.">
This is due to a combination of factors including, but not limited to, the lack of familiarity among national staff with financial management practices and procedures used by governments and donors, and insufficient control and national oversight.
This was due to a combination of different factors including, inter alia, inadequate knowledge by national staff of financial management practices and of government and donor procedures as well as insufficient monitoring and supervision at the national level.
Insufficient monitoring and supervision at the national level.">
The arms trade is rapidly spiraling out of control, and insufficient control is the result of various factors.
The arms trade is spiraling dangerously out of control, and that lack of control is the result of various factors.
Lack of control is the result of various factors.">
The working group also found serious shortcomings in the system of providing legal assistance to accused persons in need, and also drew attention to insufficient control over the actions of the police in the criminal justice process and the lack of checks and balances in the relationship between the police and the judiciary.
The Working Group also noted serious shortcomings within the system of legal aid for indigenous defendants and insufficient monitoring of the police during the course of the criminal justice process, as well as a lack of checks and balances between the police and the judiciary.
Insufficient monitoring of the police during the course of the criminal justice process, as well as a lack of checks and balances between the police and the judiciary.">
Paragraph 20 of the report notes insufficient control from New York over financial resources in other duty stations; he would like to know whether control deficiencies also existed in other areas.
Paragraph 20 of the report referred to a lack of control by New York over the financial resources at the other duty stations; he wondered whether that lack of control extended to other areas as well.
Lack of control by New York over the financial resources at the other duty stations; he wondered whether that lack of control extended to other areas as well.">
Other problems associated with the use of AMUS in the region include weak participation, biased mediators, lack of knowledge about this method, lack of willingness to reach consensus, the legally non-binding nature of any agreements reached and insufficient control for the results.
Other problems with the use of ADR in the region included weak preparation, partial mediators, insufficient knowledge of the method, lack of willingness to reach consensus, the non-binding character of any agreements reached and insufficient monitoring of the results.
Insufficient monitoring of the results.">
The Board is concerned that the slow pace of project implementation during the year indicates insufficient control their implementation, which may negatively affect the completion of activities carried out within the framework of projects and the subsequent completion of work on projects.
The Board is concerned that the slow pace in the delivery of the projects during the year indicates insufficient monitoring during implementation, and that this may negatively impact the completion of the projects" activities and the subsequent closure of the projects.
Insufficient monitoring during implementation, and that this may negatively impact the completion of the projects" activities and the subsequent closure of the projects.">
Concentration and privatization of food production, insufficient control global food prices and lack of food sovereignty, leading to displacement, loss of livelihoods, impoverishment, debt-related suicides and physical violence;
Concentration and privatization of food production, lack of control over world food prices, and lack of food sovereignty, leading to displacement, loss of livelihoods, impoverishment, "debt suicides" and physical violence
Lack of control over world food prices, and lack of food sovereignty, leading to displacement, loss of livelihoods, impoverishment, "debt suicides" and physical violence">
Insufficient control over the implementation of programs and the results obtained due to the lack of personnel, processes and tools
Insufficient monitoring of program implementation and outcomes due to lack of staff, processes and tools">
Insufficient control National Committees' policies regarding their reserves may lead to the accumulation of excessive reserves, thereby reducing the available funds for UNICEF's activities and programs.
Insufficient monitoring of the reserve policies of National Committees could lead to excessive reserve levels, reducing funds available for the support of UNICEF activities and programs.
Insufficient monitoring of the reserve policies of National Committees could lead to excessive reserve levels, reducing funds available for the support of UNICEF activities and programs.">
Insufficient control and lack of equal access to economic and financial resources, as well as lack of access to social protection, education and training, are factors that combine to exacerbate inequality and push more women and girls into poverty.
The lack of control and the lack of equal access to economic and financial resources, as well as the lack of access to social protection and to education and training, are factors that conspire to reinforce inequalities and to impoverish increasing numbers of women and girls.
The relevance of diagnosis and treatment of arterial hypertension (AH) continues to increase. Despite the large range of antihypertensive drugs available, it is not possible to achieve the necessary control of blood pressure (BP) due to many reasons: frequent dosing, side effects, inadequate dosage, etc. The review presents an attempt to create an algorithm for selecting antihypertensive therapy with the basic drug valsartan and its combinations with insufficient control and varying degrees of blood pressure increase, taking into account the risk of cardiovascular diseases and target organ damage. The basis was taken from clinical studies conducted on the Russian patient population: VICTORY - a study of valsartan and its combination with hydrochlorothiazide and a Russian observational study of the combination of valsartan and amlodipine. It has been shown that dose titration of valsartan from 80 to 320 mg/day and its combination with hydrochlorothiazide promotes successful blood pressure control in 91.0% of patients, provides a good and very good therapeutic effect in 96.9% of patients and shows a high subjective assessment of quality improvement life. The combination of valsartan with amlodipine is highly effective for hypertension of II and III degrees and high cardiovascular risk. In particular, initially higher figures for the average level of systolic and diastolic blood pressure were 167.5 ± 16.2 and 100.1 ± 9.2 mm Hg. Art. – decreased to target values in 80% of patients. Thus, an algorithm for the treatment of hypertension with valsartan and its combination with hydrochlorothiazide or amlodipine as basic antihypertensive drugs was created. At the same time, it was possible to achieve blood pressure control in 80–91% of patients with hypertension of varying degrees.
Key words: arterial hypertension, insufficient control, blood pressure, combination therapy, antihypertensive therapy algorithm.
For quotation: Zagidullin N.Sh., Sukhareva N.N. Possibilities of antihypertensive therapy in case of insufficient control of arterial hypertension // Breast Cancer. Medical Review. 2017. No. 11. pp. 780-785
Possibilities of antihypertensive therapy in inadequate blood pressure control
Zagidullin N.Sh., Sukhareva N.N.
Bashkir State Medical University, Ufa
The importance of diagnostics and treatment of arterial hypertension is only increasing with the time. Despite the existing number of antihypertensive medicines, the adequate blood pressure control is not achieved because of the variety of reasons: frequency of administration, side effects, inadequate dosages, etc. In this review an attempt was made to create an algorithm for antihypertensive therapy based on valsartan in patients who do not control blood pressure at different degrees of hypertension, taking into account risks and target organ damages. The algorithm is also based on the clinical studies conducted in the Russian population such as VICTORY study with valsartan and its combination with hydrochlorothiazide and the Russian observational study with combination valsartan and amlodipine. It has been shown that the titration of valsartan from 80 to 320 mg/day and its combination with hydrochlorothiazide contributes to the successful control of blood pressure in 91.0% of patients, leads to a good and very good therapeutic effect in 96.9 % of patients and has a high subjective assessment of the treatment. A combination of valsartan with amlodipine is effective at severe stages of hypertension and in patients with high cardiovascular risk. In particular, initial blood pressure 167.5±16.2/100.1±9.2 mm Hg can be decreased to target level in 80% of patients. Thus, the algorithm for the treatment of arterial hypertension was developed using valsartan and its combination with hydrochlorothiazide or amlodipine as the basic antihypertensive medicines to achieve blood pressure control in 80–91% of patients at different degrees of arterial hypertension.
Key words: arterial hypertension, inadequate control, blood pressure, combined therapy, algorithm for hypertension treatment.
For citation: Zagidullin N.Sh., Sukhareva N.N. Possibilities of antihypertensive therapy in inadequate blood pressure control // RMJ. 2017. No. 11. P. 780–785.
The article is devoted to the possibilities of antihypertensive therapy in case of insufficient control of arterial hypertension
Arterial hypertension (AH) is a very common pathological condition, and its prevalence in the Russian Federation reaches 45%. A number of clinical studies have shown that lowering blood pressure (BP) to recommended values, including in patients at high risk of cardiovascular disease (CVD), leads to a significant reduction in mortality. Achieving target blood pressure levels with the help of antihypertensive drugs can reduce mortality from cerebral stroke by 35–40% and coronary heart disease (CHD) by 20–25%. When taking antihypertensive drugs, you should first of all strive to strictly control blood pressure and achieve its optimal values. If the degree of blood pressure reduction is insufficient, adjustment and selection of the most effective treatment regimen is required. The attending outpatient physician, with limited time to communicate with the patient, needs disease treatment algorithms developed on the basis of available scientific evidence. It is important to take into account recommendations for the selection of therapy, its safety, and concomitant diseases. The frequency of dosing is also important: the latest recommendations give preference to a single daily dose, which significantly increases patient compliance. Therefore, a modern antihypertensive drug should have a wide range of dosages for convenient titration. Considering that 70–80% of patients require combination therapy, fixed combinations with different dosages are advisable, which would make the process of drug titration more convenient and allow choosing therapy for any degree of hypertension.
Currently, for most of the most commonly used antihypertensive drugs, an extensive evidence base has been created, based on randomized clinical trials and meta-analyses. At the same time, given the high prevalence of cardiovascular drugs in Russia, data from studies conducted in our country are of particular value.
Choosing a class of antihypertensive drug
Hypertension is a multicausal disease, the pathogenesis of which involves several systems, while the renin-angiotensin-aldosterone system (RAAS) plays a key role in the pathogenesis of cardiovascular diseases, regulating fluid levels in the body, electrolyte balance, blood pressure, etc. (Fig. 1 ). Therefore, angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) as monotherapy for mild or moderate hypertension achieve satisfactory results in 40–60% of patients, which is comparable to the effect of other antihypertensive drugs. As is known, renin coming from the kidneys converts angiotensin into angiotensin I, which, in turn, is metabolized into angiotensin II (AT II) with the help of angiotensin-converting enzyme (ACE). The action of AT II develops through interaction with angiotensin receptors type 1 (AT1): by binding to AT1, angiotensin II causes vasoconstriction, water and sodium retention and is capable of increasing blood pressure. ARBs selectively block AT1 receptors, preventing vasoconstrictor and other effects. It is important to remember that there are also angiotensin type 2 receptors, the activation of which, unlike AT1 receptors, leads to the opposite positive effects on the cardiovascular system: vasodilation, inhibition of cell growth, suppression of vascular cell proliferation, increased production of nitric oxide , inhibition of cardiomyocyte hypertrophy, etc. ARBs leave AT2 receptors intact and retain their positive effects, which is an important advantage of their pharmacological action.
In addition, the mechanism of action of ARBs provides a high safety profile for this group of drugs. By blocking AT II at the receptor level, ARBs eliminate the possibility of bradykinin accumulation and the associated cough, which often occurs when taking ACE inhibitors.
It is also important that ARBs do not have an “escape effect” of hypotensive action associated with alternative pathways of AT2 synthesis (chymase and cathepsin G), which is often found with ACE blockade. ARBs completely neutralize the effect of AT II at the last stage, turning off the corresponding receptors, which provides predictable blood pressure control for many years.
Just a few years ago, ARBs were positioned exclusively as second-line drugs that were recommended for use in cases of intolerance to ACE inhibitors; currently, more than 200 million patients take drugs in this group, which accounts for approximately 25% of antihypertensive drug prescriptions. The basis for this was the results of the LIFE and SCOPE studies, which proved the effectiveness of ARBs in preventing primarily cerebral strokes. Evidence has been obtained in favor of ARBs in major CVDs: hypertension, during and after myocardial infarction, chronic heart failure (CHF), left ventricular hypertrophy (LVH), etc. They have pronounced neuro-, vaso- and nephroprotective effects. In combination with the absence of side effects, sartans have become the most popular group of drugs not only for hypertension, but also for the other above-mentioned conditions. In addition, according to G. Mancia et al. (2001), adherence of hypertensive patients to treatment with ARBs exceeds adherence to the use of any other class of antihypertensive drugs. Good compliance is also maintained when prescribing fixed combinations of ARBs with other drugs.
The group of sartans is characterized by heterogeneity both in chemical structure and in the degree of affinity for AT1 receptors and pharmacokinetic characteristics. Of the ARBs, one of the most popular and prescribed drugs is valsartan, whose selectivity for angiotensin receptors is 24 thousand times higher than for angiotensin II receptors, which largely explains its effectiveness in clinical practice. In a meta-analysis by R. Nixon et al. Data from prospective randomized studies on 13 thousand patients were analyzed and changes in blood pressure were assessed while taking different sartans in equivalent doses for 6–12 weeks. therapy. It has been shown that valsartan at an average dose (160 mg/day) has certain advantages. Valsartan significantly better reduced both systolic blood pressure (SBP) (by 15.32 mm Hg) and diastolic blood pressure (DBP) (by 11.33 mm Hg) than losartan (by 12.01 and 9. 37 mmHg respectively). Compared with the average dose of irbesartan (150 mg/day), a significantly greater effect of valsartan (160 mg/day) on SBP and DBP was shown. The KYOTO HEART study followed 3042 patients with poorly controlled hypertension and high cardiovascular risk for 3.3 years. After adding valsartan, there was a significant reduction in the incidence of cardiovascular and cerebrovascular outcomes by 45%, including myocardial infarction by 49% and stroke by 45%. The hypotensive effect of valsartan increased with increasing dose from 80 to 320 mg, which was also accompanied by an increase in the frequency of achieving target blood pressure. When analyzing the results of 9 clinical studies (n=803), the rate of restoration of target blood pressure when taking valsartan was studied: at a dose of 80 mg and 160 mg, the effect was achieved after 1 month, and when adding hydrochlorothiazide to valsartan, after 3 weeks. .
Thus, valsartan and its combinations can be a scientifically, pharmacokinetically and clinically sound choice when creating an algorithm for selecting therapy for insufficient control of hypertension.
Algorithm for selecting therapy for insufficient control of hypertension
Let us consider possible algorithms for prescribing antihypertensive therapy, taking into account modern requirements and the availability of evidence, paying attention to the Russian patient population (Fig. 2).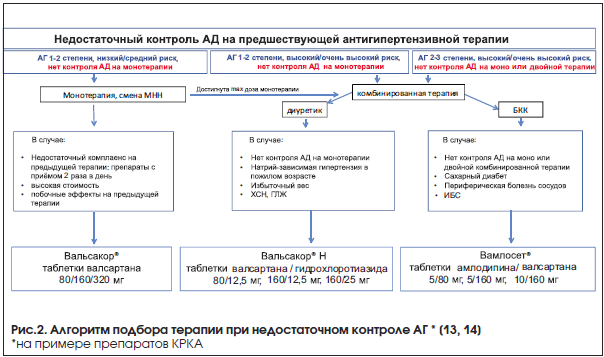
1. Stage I–II hypertension of low/moderate risk, no control on monotherapy. The following options to increase efficiency should be considered.
A. Further dose titration. This option is not possible if: (1) the maximum dose of the drug has been reached and (2) further titration is associated with an increased risk of side effects. In both cases, it is advisable to change the antihypertensive drug (point B).
B. Change of drug. Choosing an ARB can reduce the number of side effects and increase adherence to therapy. Also, the availability of a large assortment of drugs, in many cases, allows us to revise the cost of therapy downwards, while maintaining the high quality of therapy. Suppose one antihypertensive drug taken 2 or more times a day, such as enalapril, is replaced by a once-daily drug. As is known, when taking drugs 2 times a day, compliance is reduced by 10–15% compared to a single dose. The occurrence of side effects, such as dry cough when taking ACE inhibitors, causes caution, mistrust in the patient and reduces adherence to treatment. In this case, it is recommended to use an ARB with minimal side effects - valsartan, which in most cases leads to an effective reduction in blood pressure. Thus, the VICTORY study showed that replacing previous ineffective antihypertensive therapy (most often enalapril and captopril) with monotherapy with valsartan 80, 160 or 320 mg (Valsakor®, KRKA) led to a decrease in mean blood pressure from 156.6/95.6 mm Hg Art. up to 130.1/80.9 mm Hg. Art.
2. Stage I–II hypertension, high/very high risk, no blood pressure control on monotherapy. As a rule, monotherapy is not able to provide a sufficient reduction in blood pressure and organ protection. To adequately control blood pressure and minimize cardiovascular complications (CVC), combination therapy is required. A diuretic in combination therapy significantly enhances the effect of the first drug (including valsartan) and is desirable for sodium-dependent hypertension, old age, reduced ejection fraction (with CHF), LVH and excess body weight. Even in the presence of such a potentially unsafe condition with respect to diuretic monotherapy as diabetes mellitus (DM), hydrochlorothiazide (HCTZ) in combination with an ARB showed a significant reduction in blood pressure and good tolerability. In this case, we have at our disposal a combination of valsartan and HCTZ: tablets Valsacor® N 80 (80/12.5 mg), Valsacor® N 160 (160/12.5 mg) and Valsacor® ND (160/25 mg), which showed their effectiveness and safety in the already mentioned VICTORY study.
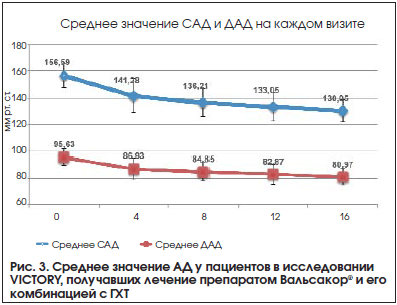
The purpose of the randomized, open, prospective, international multicenter study VICTORY (Czech Republic, Russia, Slovenia, Croatia, Ukraine participated) was to evaluate the effectiveness and safety of valsartan monotherapy and its fixed combination with HCTZ in different dosage regimens: Valsacor® 80, 160, 320 mg, Valsacor® H 160 (valsartan 160 mg + HCTZ 12.5 mg), Valsacor® H 320 (valsartan 320 mg + HCTZ 12.5 mg) – in achieving the target blood pressure level in patients with hypertension of I–II degree, in whom symptomatic hypertension was excluded . The study included 365 patients, including 130 patients from 8 cities in Russia. In the Russian part of the study, the starting dose of valsartan depended on previous antihypertensive therapy: for primary patients 80 mg (Valsakor® 80 mg) with randomization into 4 parallel groups. For patients receiving antihypertensive therapy at the time of screening, Valsacor® 160 mg was prescribed after a 7-day washout period. The duration of therapy was 16–20 weeks. with 5 visits. In patients with hypertension aged 54.6±12.0 years, clinical blood pressure at the time of inclusion in the study was 156.6/95.6 mmHg. Art. By the 4th week of monotherapy with valsartan 80 or 160 mg, blood pressure decreased to 141.3/86.9 mmHg. Art. Titration of valsartan or the addition of HCTZ to the 8th week contributed to a further decrease in blood pressure to 136.2/84.8 mm Hg. Art. By the 16th week of treatment, a decrease in blood pressure to 130.3/80.9 mm Hg was observed. Art. (p<0,000001). В результате терапии валсартаном и его сочетанием с ГХТ целевые значения АД были достигнуты у 91% пациентов, участвовавших в исследовании. Терапевтический эффект оценивался как хороший и очень хороший у 96,9% пациентов. Общая клиническая эффективность оценивалась как чрезвычайно высокая, очень высокая и высокая у 95,3%. Нежелательные явления отмечались у 7,1% больных. Наиболее частыми нежелательными явлениями были головная боль (1,9%), тахикардия (1,6%), головокружение (1,6%), слабость (1,6%). Процент пациентов, имевших отклонения от нормальных значений уровней глюкозы, креатинина и калия, не увеличивался с начала исследования до 16-й недели лечения.
Thus, valsartan in monotherapy and in combination with HCTZ significantly reduced the level of systolic and diastolic blood pressure to normal values (Fig. 3). It is especially important that the reduction in blood pressure occurred both in primary patients and in patients with stage I–II hypertension who were already taking other antihypertensive therapy before the start of the study.
3. Stage II–III hypertension when the target blood pressure level was not achieved on previous mono- or dual therapy. Such patients belong to the category of high and very high risk of cardiovascular complications. In this case, the most effective combination antihypertensive therapy with a rapid onset of the hypotensive effect should be used. Such a combination could be a combination of valsartan and the calcium channel blocker (CCB) amlodipine, especially since this combination showed good results in a Russian observational study. Since the bulk of adverse cardiovascular events occur in the morning, it is especially important that the effect of antihypertensive drugs extends to the night and morning, and not only reduces the so-called office blood pressure. Valsartan has a long half-life of 9 hours, noticeably reduces blood pressure after 2 hours, and the duration of action is 24 hours or more. The calcium channel blocker amlodipine is also a daily action drug. The half-life of repeated administration is 45 hours. The antihypertensive effectiveness of the combination of valsartan and amlodipine has been shown in a number of studies, including those conducted in Russia.
An open Russian observational study included 2874 patients with hypertension (mean age 55.7 years, 46.8% men, 53.2% women). Inclusion criteria were uncontrolled hypertension. 89.7% of patients had already received antihypertensive therapy before entering the study; the rest were prescribed therapy for the first time. The majority of patients were classified as high and very high risk for cardiovascular complications. All patients were titrated with a combination of valsartan 80 and 160 mg with the addition of amlodipine 5 or 10 mg. The initial blood pressure level (167.5±16.2/100.1±9.2 mmHg) significantly decreased by 38.9/19.6 mmHg. Art. (p<0,0001) в течение 12 нед. лечения (рис. 4). Целевой уровень АД <140/90 мм рт. ст. достигнут у 80% пациентов. Особо следует подчеркнуть, что до исследования большинство пациентов уже принимали терапию (антагонисты кальция, иАПФ, другие БРА, бета-блокаторы и диуретики) и она не была эффективной. Это говорит о том, что назначение комбинации валсартана с амлодипином дополнительно снижает АД не только при неэффективности монотерапии, но и при неэффективности двойной терапии различными классами препаратов. Учитывая метаболическую нейтральность препаратов, комбинация валсартана с амлодипином особенно подойдет пациентам с СД, кроме того, способность амлодипина благоприятно влиять на атеросклеротическую бляшку делает данную комбинацию препаратом выбора для пациентов с периферической болезнью сосудов. Также необходимо учитывать благоприятное влияние амлодипина на спастический компонент стенокардии. В предлагаемом алгоритме можно выбрать одну из 3-х дозировок комбинации амлодипина с валсартаном: таблетки Вамлосет® 5/80, 5/160, 10/160 мг.

Conclusion
Thus, an algorithm has been developed to overcome insufficient blood pressure control in patients with hypertension of varying degrees (see Fig. 2):in the absence of blood pressure control during monotherapy of stage I–II hypertension in patients with low/moderate risk of cardiovascular events– use of valsartan (Valsakor® 80/160/320 mg);
in the absence of blood pressure control during monotherapy for stage I–II hypertension with a high/very high risk of cardiovascular events– use of a combination of valsartan with HCTZ: Valsacor® N 80 mg, Valsacor® N 160, Valsacor® ND;
in the absence of control with monotherapy or in case of ineffectiveness of previous dual therapy in patients with stage II–III hypertension and a high/very high risk of cardiovascular complications - a combination of amlodipine and valsartan (Vamloset® 5/80, 5/160, 10/160 mg).
The drugs proposed in the algorithm not only have an extensive evidence base, a good safety profile, and provide additional blood pressure control in case of ineffective previous antihypertensive therapy, but have also proven themselves well in Russian patients.
Literature
1. Belenkov Yu.V., Chazova I.E. The first Russian national multicenter study - ROSA (Russian Study of Optimal Reduction of Blood Pressure) // Arterial Hypertension. 2005. T. 9. No. 5. pp. 234–238.
2. Fox K.M. Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomized, double-blind, placebo-controlled, multicentre trial (the EUROPA study) // Lancet. 2003. Vol. 362. P. 782–788.
3. Lubsen J., Wagener G., Kirwan B.A. et al. Effect of long-acting nifedipine on mortality and cardiovascular morbidity in patients with symptomatic stable angina and hypertension: the ACTION trial // J Hypertens. 2005. Vol. 23(3). P. 641–648.
4. Mancia G., De Backer G., Dominiczak A. et al. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension // Hypertens. 2007. Vol. 25(6). P. 1105–1187.
5. Dahlof B., Devereux R.B., Kjeldsen S. et al, for the LIFE Study group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomized trial against atenolol // Lancet. 2002. Vol. 359. P. 995–1003.
6. Lithell H., Hansson L., Skoog I. et al. The Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trial // J Hypertens. 2003. Vol. 21. P. 875–886.
7. McNenes G.T. Angiotensin II antagonism in clinical practice: experience with valsartan // J. Cardiovascular Pharmacol. 1999. Vol. 33. Suppl 1. P. 29–32.
8. Mancia G. Clinical differences among angiotensin II receptor antagonists // Blood Press Suppl. 2001. Vol. 2. P. 19–24.
9. Nixon R.M., Muller E., Lowy A., Falvey H. Valsartan vs. other angiotensin II receptor blockers in the treatment of hypertension: a metanalytical approach // Int J Clin Prac. 2009. Vol. 63(5). P. 766–775.
10. Sawada T., Yamada H., Dahlof B., Matsubara H. for the KYOTO HEART Study Group. Effects of valsartan on morbidity and mortality in uncontrolled hypertensive patients with high cardiovascular risks: KYOTO HEART Study // Eur. Heart J. 2009. Vol. 30. P. 2461–2469.
11. Pool J.L., Glazer R., Chiang Y.T. et al. Dose-response efficacy of valsartan, a new an-giotensin II receptor blocker // J Hum. Hypertens. 1999. Vol. 13. P. 275–281.
12. Weir M.R., Levy D., Crikelair N. et al. Time to achieve blood–pressure goal: influence of dose of valsartan monotherapy and valsartan and hydrochlorothiazide combination Therapy // Am J Hypertens. 2007. Vol. 20. P. 807–815.
13. Diagnosis and treatment of arterial hypertension. Clinical recommendations. M. 2013.
14. European clinical guidelines for the treatment of arterial hypertension. ESH/ESC. 2013.
15. Chazova I.E., Martynyuk T.V. The first results of the international clinical study VICTORY: the effectiveness and safety of antihypertensive monotherapy with valsartan and its fixed combination with hydrochlorothiazide in different dose regimens in patients with arterial hypertension of the 1st and 2nd degrees // Systemic hypertension. 2015. T. 12. Issue. 2. pp. 71–82.
16. The efficacy and safety of valsartan and combination of valsartan and hydrochlorothiazide in the treatment of patients with mild to moderate arterial hypertension – VICTORY. Final report. Data on file. Krka d.d., Novo mesto, Slovenia, 2015.
17. Weir M.R., Neutel J.M., Bhaumik A. et al. The efficacy and safety of initial use of irbesartan/hydrochlorothiazide fixed-dose combination in hypertensive patients with and without high cardiovascular risk // J Clin Hypertens. 2007. Vol. 9 (12 Suppl 5). P. 23–30.
18. Kereiakes D.J., Chrysant S.G., Izzo J.L. et al. Olmesartan/amlodipine/hydrochlorothiazide in participants with hypertension and diabetes, chronic kidney disease, or chronic cardiovascular disease: a subanalysis of the multicenter, randomized, double-blind, parallel-group TRINITY study // Cardiovasc Diabetol. 2012. Vol. 30(11). P. 134.
19. Karpov Yu.A., Chazova I.E., Vigdorchuk A.V. Efficacy and safety of a fixed combination of amlodipine and valsartan in the treatment of arterial hypertension in real clinical practice: results of the Russian observational study EXTRA-2 // Systemic hypertension. 2010. No. 4. P.18–26.
20. Destro M., Scabrosetti R., Vanasia A. et al. Comparative efficacy of valsartan and olmesartan in mild-to-moderate hypertension: results of 24-hour ambulatory blood pressure monitoring // Adv Ther. 2005. Vol. 22(1). P. 32–43.
21. Ruilope L.M., Heintz D., Brandao A.A. et al. 24-Hour ambulatory blood-pressure effects of valsartan and hydrochlorothiazide combinations compared with amlodipine in hypertensive patients at increased cardiovascular risk: a VAST sub-study // Blood Press. Monit. 2005. Vol. 10 (5). P. 85–91.
Probably no one needs to be convinced that every person needs a sense of control over their own life. We encounter manifestations of this need at every step.
Given the need for control present in all people (to a greater or lesser extent), it can be argued that compulsive patterns often associated with depression. Any compulsive stereotype is an attempt win anxiety, fear and uncertainty- and, of course, depression – by establishing repetitive and even ritualistic actions, which are intended to be a way to cope with certain aspects of life experience.
Let's look at the most typical features compulsive individuality. Such a person, as a rule, attaches great importance to morality, principles and etiquette. Why such a strong attachment to principles and values? The feeling of loss of control (and at the same time anxiety, fear, uncertainty) is very strong if at least one detail of any experience is not taken into account in the personal "code of conduct".
The rules that provide an individual's choice are closely related to the value systems in question, especially those that limit the ability to respond optimally in a particular situation. Inappropriate stereotypes related to control (i.e., those that weaken the ability to find the optimal response in a given context) are often inadvertently reinforced by individuals playing an important role in the socialization process.
Map of yourself
Given the importance of previously instilled beliefs regarding issues of control, power, responsibility and other issues relevant to depression, a task called composing may be very useful. "cards of oneself."
1. The patient is advised to determine the values on which the range of choices available to him depends. The client should make a list of problems related to both personal and public spheres, such as power, responsibility, prejudice, death penalty, abortion. The longer the list, the better.
2. Opposite each point, the patient draws a continuum, the ends of which represent opposing points of view on a given problem. For example, for the position “need for control” a continuum can be drawn, one of the poles of which will be defined as "great need for control" and the other - “low need for control.”
3. The client should then mark items on each axis that represent the viewpoints of those important to him. Thus, he is faced with the need to reflect on the views of the people who played a large role in the process of his development. As a result, the client becomes convinced whether these opinions were obvious to him or whether he had difficulty identifying them. In both cases, the result turns out to be interesting and useful.
4. The next stage of the task is as follows: the client is asked to indicate on each continuum the point that corresponds to his own opinion. Having thus determined his position, the patient can compare it with the position of the people who had the greatest influence on him.
Difference or agreement can provide rich material for reflection. The therapist then asks the client to imagine behavior consistent with each of these life positions.
5. Finally, the client should describe the types of behavior that are completely inconsistent with these views. Thanks to this exercise, the patient begins to understand the need to understand his own value system and behavior consistent with this system. An additional advantage of this strategy is the chance to avoid situations in which the client would be forced to speak out for views that he does not accept.
At any stage of the intervention, the therapist has the opportunity to identify the client's values and life beliefs regarding the issue of control and power. Particularly noteworthy are those values and views that deprive an individual of faith in the ability to control his own reactions to a situation.
Loss of sense of control
Since controlling one’s own choices performs an essential function in a person’s life, it is quite obvious that disruption of this activity has a significant impact on the quality of existence of the individual. Violations in this dimension can manifest themselves in different ways: in the form of a repeated tendency to lose control over a situation or in a tendency to control it excessively.
A person who does not have enough control over the situation is characterized by helplessness, typical of thinking " victims" Finding himself in a position in which, by taking an appropriate action, a person would have a chance of obtaining positive results or avoiding a threat, he refuses the intervention.
The development of the mechanism of such behavior is perfectly illustrated by the experiments of Martin Seligman (1973., 1974, 1983), when in a situation that could theoretically be handled, individuals showed passivity and helplessness.
Participants in the experiment were exposed to negative impulses that were beyond their control. Regardless of the efforts made, escaping from negative factors was impossible. Later, the situation changed: there was a chance to avoid negative impacts, but the subjects continued to do nothing, based on a previously formed belief (which had already lost its relevance) that all efforts would be in vain. Seligman called this phenomenon "learned helplessness."
A person who exhibits a tendency to be overly controlling will try to control the situation, even if in reality it is outside his sphere of influence. This personality type is characterized by blurring the line between hope and reality.
A person knows what he wants and tries to achieve it, but as a result, all this leads to an increase in stress and depression, because the goal eludes the person. Since he does not understand that the goals he has set are unrealistic, and he explains his failure by his own mediocrity, all this often ends in depression for him.
With regard to the diagnostic categories described in the fourth section, a person with insufficient control of the situation (the “victim” type) is generally characterized by the following traits:
global thinking,
focus on others
openness,
people orientation
extrapunitiveness,
poorly defined value system,
unstable sense of self-worth,
high reactivity,
orientation to the past and
low ability to dissociate.
A person characterized by excessive control, i.e., trying to influence what is outside his sphere of influence, shows a tendency to excessive feelings of guilt, self-blame, concrete and linear thinking, self-directedness and task orientation.
In relation to the above patterns, which are universally observed in those suffering from depression, the basis of therapy is to discover and enable the client to use his complementary parts (abilities).
Typical problems associated with control disorders
The above description of deviations - in one direction or another - in the sphere of the sense of control is of a general nature. Here are a few examples that illustrate problems common in individuals with perceived control disorders.
Insufficient control: case 1
Jenny, a thirty-year-old university employee, had direct contact with students through her work. The woman decided to undergo therapy due to depressive feelings, anxiety and low self-esteem. Her problems have been going on for five years now. Jenny associated them with the divorce, which nevertheless occurred, despite her efforts to save the marriage at all costs. The patient complained of her inability to give up things and people with whom she was associated. As evidence of this, she provided the following fact:
Jenny worked in a job she didn't like, in a place where she was underappreciated; the woman also claimed that she was unable to think about her ex-husband in the past tense. She referred to problems arising from her affair with a foreigner who had studied at her university for some time. He was going to marry a compatriot in his country, which Jenny openly admitted. She hoped that her partner would change his mind and stay with her forever. Jenny had the opportunity to change her job and partner.
However, instead of taking control of the situation that had caused her so much suffering, she allowed things to deteriorate at work and made more and more demands on a man who had no plans to join his life with her and was determined to eventually leave her .
The woman accepted the position of the victim, and as a result of this, the feeling that she herself makes decisions in her life left her. Jenny believed that by staying in her chosen positions and increasing pressure from her partner, she would eventually be able to achieve recognition and win his love. These are typical expectations of a victim hoping for a miraculous healing.
Insufficient control: case 2
Twenty-six-year-old Jim complained of depression, excessive feelings of guilt, failure in relationships with women, and low self-esteem (his case was already described in section seven). In his statements, he moved from angry complaints about the environment that had used him in the past to desperate self-accusation of a passive attitude towards current events.
It emerged from the conversation that Jim was the only man in the family (his mother, in addition to her only son, was also raising two daughters). The patient recalled events from his early youth when his mother responded to his question regarding sex with a physical intervention, which was supposedly intended to explain to the guy how his body behaved.
Jim experienced shame and guilt, and as time passed, he became increasingly conflicted by the messages his mother was conveying to him, such as the double bind. After the mentioned episode, the mother often behaved provocatively, making unambiguous hints to her son, and when he answered them, she reproached him for shamelessness and indecent thoughts.
Jim spent many years in seminary preparing himself for the priesthood, but - much to his mother's displeasure - he dropped out, which made him even more guilty. Jim saw a therapist wanting to release the anger he was experiencing and gain more self-confidence. He hoped that this would help him establish proper connections with women, because he believed that in the few relationships that he had already experienced, he was used: his partners deceived him, lured him out of money.
It was obvious that Jim saw himself as a victim. He felt the noose being tightened around his neck; From his mother he received messages like double entanglements, women used him, and, in general, he felt that he had no control over his own life and feelings.
The position “you can’t trust anyone” means an existence limited to only one dimension, excluding an intimate relationship with another person. Jim did not feel able to have any control over his relationships with his environment; he was also unable to properly assess the responsibilities of other people. He was “lost” in women, perceiving them globally and completely uncritically – and as a result, he was often offended. It's not hard to guess that Jim, the victim type, had very low self-esteem. He lacked an understanding of the motivations of others and the styles of dealing with life's problems, which is why he was so easy to exploit.
Overcontrol: Case 1
Kriv, a 45-year-old man, consulted a therapist for depression, uncontrollable outbursts of anger, and worry about the future. He was a scientist who worked in a government agency for over twenty years. Among his superiors and colleagues, he gained a reputation as a person gifted with an extraordinary ability to solve problems.
His sense of self-worth came mainly from the fact that he managed to work on a project that no one else could handle until he received a result that was certified by his superiors. Not long ago he was entrusted with an extremely difficult task, and Kriv set about implementing it, although he did not have a sufficient number of workers, and the time allotted for the task was decidedly short.
The situation had outgrown his capabilities. He was overcome by a feeling of dissatisfaction, and then depression. He stopped interacting with people, could not concentrate, and began to view the organization of his department so negatively that he demanded restructuring to improve its performance.
Keys's opinion was ignored; most likely, the scientist’s employees perceived his attacks as manifestations of temporary irritability and dissatisfaction, which it would be better to simply wait it out. As successive attempts to find support were met with indifference, Keys’s feeling of loneliness and depression grew.
Keys's reputation rested on his self-created vision of himself as a "miracle worker," the Superman of technology. His ambition and sense of duty were undoubtedly admirable, but unfortunately he failed to recognize the limits of his own capabilities. He continued to take upon himself full responsibility for a task whose completion depended on factors beyond his sphere of influence.
He tried to control the system, although he was only part of it, and he was visited by painful but inevitable disappointment. It was only when he realized his limitations and learned to refuse enterprises beyond his control that Kriv realized that, despite his education and intelligence, he could not achieve everything he wanted.
Overcontrol: Case 2
Forty-year-old Koren sought help from a therapist shortly after a failed suicide attempt by overdosing on sedatives. This event took place immediately after a serious disappointment had befallen him.
For twenty years he worked as an engineer in a well-known company. All these years he had been successfully moving up the career ladder, but he had the impression that this rise was happening too slowly.
It seemed to him that the company underestimated his noble aspirations, creative approach to work and loyalty. However, Koren hoped that if he continued to be an exemplary worker, his efforts would eventually be rewarded.
He even earned a degree in counseling psychology, capping off his decades-long interest in human behavior. He hoped that improved qualifications would provide him with a promotion - and indeed, he received certain encouraging hints.
When the company hired someone from the outside for this position, Koren’s despair was so deep that he tried to take his own life.
I met him a few days later, he was depressed, had difficulty holding back his tears, Koren reproached himself for selfishness, which had driven him to the point where he forgot about his responsibilities towards his family and wanted to die.
It was obvious that Koren had an excessive sense of responsibility, and that he was convinced that he could decisively influence the perception of those around him and make people see him as an indispensable worker, an exemplary father, a good husband, etc.
His attempt to subjugate the system ended in defeat. Koren assumed that noble aspirations should be rewarded, loyalty should be valued, and creativity should be recognized. He was very surprised when, during the first conversation, I asked him:
“Where did you get this from? Has your firm ever rewarded behavior like this?” Coren believed that his superiors were guided by the same value system as him; the patient could not bear that the reaction of his superiors was different from his expectations.
If Koren accepted their rules of the game, he would easily understand that how/how others perceive him is beyond his control. And then he could direct his creative energy in a different direction, where it would be appreciated.
What is the level of control?
A starting point for helping the client identify the quality and limits of the impaired sense of control is a structured exercise called: “What is the level of control?”
The patient makes a list of his usual actions and events of everyday life (such as arguing with friends about politics, talking with his boss about professional topics, teaching children, etc.). The patient tries, as far as possible, to determine the purpose of each action or event.
Then he himself, using a ten-point scale, determines to what extent he controlled the course and result of the action. After which the client needs to find out what was used as the basis for determining the degree of control over this situation. The therapist should note whether the client has difficulty recognizing goals and control mechanisms, and also note how strong the client's sense of control is in various situations of daily life.
0 Rating 0.00 (0 Votes)
. - ed.
I would like to see that brilliant professor who will come to the entrance examination and find a talented applicant among those who cannot perform simple standard tasks. All these are fairy tales about a white bull. Are the assignments imperfect? Let's make them better.
Let's take the bull by the horns and name the main problem. This is not enough control. A GOOD USE IS A HONEST USE.
I would venture to say that an unpleasant situation has developed - the upper classes cannot, the lower classes do not want to.
I'll start from the bottom. In the first years of the Unified State Examination, there was a clear position among educators. We need to help the children of teachers, we need to help the children of leaders. It was such an interesting fight. In the first year of the mass Unified State Examination, the package included only 7 different options in 15 papers. The impression was created that it was possible to organize mass assistance to the right people. And now, in the glorious city on the Don, 4 special centers for conducting the Unified State Exam are being organized. And there was a puncture - there were many more options that year - there were not enough specialists. They only helped the absolutely necessary people.
By the way, at the regional conference after the Unified State Exam 2004, one of the speakers analyzed the implementation of tasks A and B in rural areas.
It was proven that in one of the small rural areas, where all students were placed at one point for the Unified State Examination, interesting events took place.
Those tasks, even complex ones, to which a specialist could immediately give the correct answer, were completed significantly higher than in all other rural areas. But simple tasks that require time to calculate were performed worst in all rural areas. The heads of education in this area were given a dressing down. But, apparently, the lesson was not useful. By the way, it is now impossible to obtain such materials for research.
Now, if you'll excuse me, let's move on to the top. It seems that in words everyone is in favor of an honest Unified State Examination.
But variant leaks happen every year. What, you can’t restore order?
We are told that there are thousands and thousands of different options, and the leakage of one option is not significant. I beg to differ. Let's take the Unified State Examination in mathematics. After completing the simpler tasks and completing their answers and solutions in section C, there remains approximately an hour and a half to complete 3-4 complex tasks. If there is no information leakage, then for the student these tasks are unsolved problems. How many unsolved problems can be solved in an hour and a half?
I argue that either a genius or a schemer can get a 100 in math.
Both of them need to be taken by the hand and specifically worked with them. Next note. Is it necessary to conduct an early Unified State Examination in April? We are told that this is necessary for athletes and some others, for example, for the children of diplomats who need to go abroad (this is not a joke - I heard it myself at a regional conference).
But really, these early exams, if they are really necessary, cannot be taken under special control? There are some shenanigans going on there.
In 2009, they sent me scanned versions of the early Unified State Exam, where not only the numbers were written, but also notes to which specialist they were sent for decision. This year the numbers have already been cut, but the fraud remains.
By the way, it is still possible to identify the schemers. There would be a desire.